Chapter: Venous malformations
Article: 5 of 13
Update: Mar 25, 2021
Author(s): Barbera, Letterio Christian
The imaging techniques available, such as duplex sonography, computed tomography, magnetic resonance imaging, digital subtraction angiography and phlebography, enable a venous malformation to be diagnosed accurately and rapidly.
Since each patient has a very unique expression of the disease, a differentiated and therefore time-consuming analysis of the imaging studies is necessary. Extension, infiltration in depth, appearance, contrast enhancement, structural changes to the superficial and deep veins, subcutaneous tissue, muscle and bone are examined. The extension in length (which parts of the body, how many cm?), in circumference (circular, lateral only?) and estimated total volume (small, medium, large) are noted. A more precise determination of the extension of a large venous malformation is usually not possible in everyday clinical practice, as it consists of countless irregular structures. Furthermore, the fact that the degree of filling is variable depending on body position, degree of activity, hormonal situation, compression therapy and room temperature must be taken into account.
Nevertheless, an attempt should be made to describe the extension as precisely as possible. This also includes observation of infiltration in depth: subcutaneous, subfascial, intra-articular, with displacement of the peritoneum, the pleura or the oral mucosa. Often it is precisely the VM parts in the deeper tissue layers and not the easily accessible subcutaneous malformations that are responsible for the symptoms.
The description of the appearance (e.g. oval, large-lumen, ramified, multilobulated) is important both for planning the intervention and for recognition of the venous malformation during the intervention. If, for example, the knee joint is sore and the venous malformation extends intra-articularly according to the MRI, these parts and not the adjacent malformations in the subcutis should be sclerosed.
Visualization of large-lumen communicating veins from the venous malformation into the deep venous system is particularly important, since this determines not only the risk of thromboembolism, but also the effectiveness of sclerosing treatment. The focus is on vascular imaging, therefore the administration of contrast agents is always necessary. In view of the slow blood flow in a venous malformation, the late phase, also called the venous phase, should be recorded. The venous malformation is usually not visualized until after the regularly developed venous system.
Before imaging is performed, it is advisable to consult with the radiologist and discuss the respective case from a clinical perspective. The more precise the clinical question is, the more targeted the diagnostic study becomes. It is less about beautiful “esthetically” valuable images of the venous malformation and more about detailed imaging of immature and regular vessels and their relation to each other.
Imaging is important for the detection or exclusion of aplasia and dysplasia of the accompanying deep venous system. The absence of deep veins or their dysplasia requires caution in invasive therapeutic procedures. The morphology and function of the great and small saphenous veins are equally assessed. They should only be removed in clinically relevant cases of insufficiency. Unfortunately, in practice these vessels are often treated while the actual venous malformation remains undetected. This worsens the congestion symptoms in the lower extremity.
In the arms, the superficial and deep veins (= epi- and subfascial veins) are clinically less significant, as the hydrostatic pressure is lower. Nevertheless, they should be spared in the course of interventions.
Cross-sectional imaging allows identification of the tissue that accounts for the difference in circumference (fatty tissue? lymphedema?). A subcutis that is thicker and coarser compared to the unaffected side suggests the simultaneous presence of an LM. A narrower muscle layer, on the other hand, indicates an associated partial hypoplasia (immobilization due to pain) and the need for intensive physiotherapy. It is rare for an extensive venous malformation to be intraosseous and even rarer for it to have any clinical significance. However, in view of the considerable variability of the findings, any bone involvement by the venous malformation should be described.
Different imaging techniques are available and are necessary for treatment, if indicated.
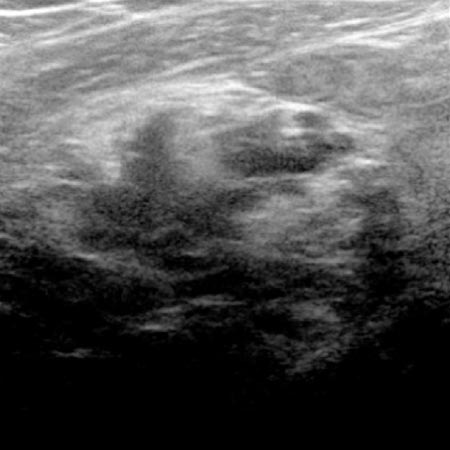
Sonography allows good visualization of venous malformations in the soft tissue. Extension in depth (subcutis, musculature), volume distribution and possibly the presence of thrombosed parts and phleboliths can be recorded in B-mode. At the same time, color coding enables the distinction to be made from LM, in which no blood flow can be detected at all. A slow blood flow in a venous malformation can often only be detected by manipulation (compression of the adjacent soft tissues by hand). The color gain should be increased up to just before aliasing effects in order to detect even very slow blood flow. Form and function of the superficial and deep veins of the affected limb are also examined and documented. However, changes in the deep vein system are not always detected, so that further diagnostics (usually MRI) should be arranged in these cases.
The disadvantages of sonography are the operator dependence, the insufficient image documentation and the imaging of only limited areas. It is a good method for diagnosis and therapy planning of smaller venous malformations (diameter < 5 cm) as well as for follow-up.
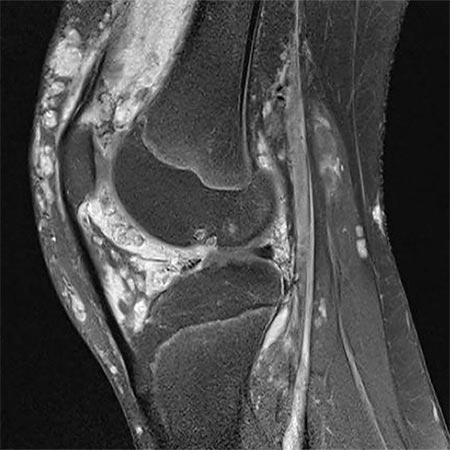
High spatial resolution, good soft tissue contrast, three-dimensional image reproduction and development of specific examination protocols for tissue perfusion and vascular imaging render MRI the gold standard in venous malformation imaging. There is an indication for this if the congenital vascular malformation is extensive and/or painful, i.e., whenever invasive treatment is considered. However, findings of little clinical relevance do not require this type of diagnostic study. In particular, children should not receive unnecessary examinations under anesthesia if invasive therapy is not being considered. In addition to the justifying indication, appropriate know-how in the selection of image sequences is essential for the success of the examination. In a team discussion between clinicians and radiologists, the relevant questions should be clarified, and the appropriate protocol should be chosen. The examination is performed without and with contrast medium as magnetic resonance angiography (MRA), so that the venous malformation can be distinguished from an LM, since the latter does not enhance. A venous malformation is strongly hyperintense (white) in the T2-weighting, especially after fat suppression. In the native T1-weighted images it is hypointense, similar to musculature. After administration of contrast medium it shows slow but almost complete enhancement of the lesion.
This sectional imaging technique provides three-dimensional images with a spatial resolution comparable to that of MRI, but with the disadvantage of radiation exposure and lower soft tissue contrast. Accordingly, it is generally only used when there are contraindications to MRI (claustrophobia, non-MRI-compatible metal implants). The venous malformation is isodense to musculature and enhances entirely with the contrast medium. Calcified phleboliths are easily detected in CT.
Modern cross-sectional imaging techniques (MRI, CT) and especially MR angiography have replaced DSA in the diagnosis of venous malformations. Use of DSA is very rarely indicated in mixed forms of venous malformations with pronounced arteriovenous fistulas, when it has to be decided whether the arterial or venous component of the malformation is the main cause of the symptoms. Otherwise, it is not indicated for a suspected venous malformation. On the other hand, DSA plays a relevant role in the assessment of an AVM.
Ascending phlebography is used to clarify aplasia and dysplasia of the deep venous system when duplex sonography and MRI do not provide a reliable assessment. The indication is therefore limited to very specific questions. It is during sclerotherapy of a venous malformation that phlebographic imaging by direct puncture is essential.