Chapter: Thrombosis and thrombophlebitis
Article: 1 of 4
Update: Mar 24, 2021
Author(s): Wohlgemuth, Walter A.
Both phlebothrombosis, also known as deep vein thrombosis, and thrombophlebitis (superficial venous inflammation) are based on the formation of a blood clot (thrombus) within a venous vessel. These blood clots are formed by pathological processes such as damage to the vessel wall, increased clotting and slowed blood flow.
Some of these factors that promote thrombus formation are classically referred to as Virchow's triad:
However, in addition to the above characteristics, intrinsic coagulability and the degree of activation of the coagulation system also play an important role.
In phlebothrombosis, this concerns blood clot formation within a truncal vein or a deep conducting vein, which has a direct venous blood outflow via a larger draining vein to the interior of the body and eventually, for example, to the pulmonary circulation. In the case of phlebothrombosis, the clot can therefore migrate centrally (thromboembolism), e.g., directly to the right heart and from there to the pulmonary arteries, thus potentially causing a pulmonary embolism.
The thrombus can also block the outflow of venous blood locally in a part of the body (e.g., a leg if there is thrombotic blockage of the iliac vein), resulting in a congestive build-up of venous blood.
Thrombophlebitis, on the other hand, affects more circumscribed, superficial portions of the venous system, and the risk of thromboembolism is smaller here as there is normally no central outflow.
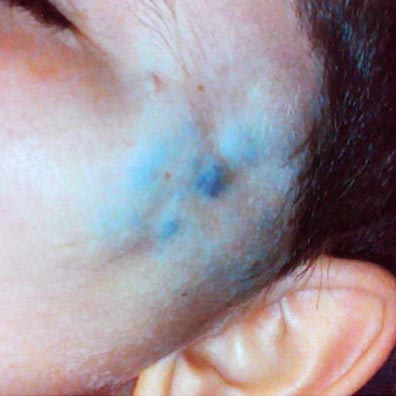
Patients with venous malformations, in particular, have a significantly increased tendency to develop phlebothrombosis and thrombophlebitis. In these patients, the vein walls are pathologically altered, the veins themselves are often markedly dilated, and the blood flow velocity is greatly reduced. If there are connections from the venous malformation to the body's draining truncal venous system via communicating or drainage veins, the risk of thromboembolism is substantially increased. This can pose a significant risk to patients in their long-term course.
In thrombophlebitis, on the other hand, this blood clot formation is more circumscribed and usually affects smaller veins, mainly those located superficially under the skin or within a venous malformation. In this situation there may not be a direct connection to the deep, draining vein system. Thus, a blood clot usually cannot reach the right heart and pulmonary arteries. There is also no relevant congestion of the outflowing venous blood.
This distinction is very important because the most significant, serious complications (thromboembolism and pulmonary embolism, congestive dermatitis, chronic venous insufficiency) arise primarily in phlebothrombosis, which therefore requires urgent treatment.
The thrombi formed in the veins or venous malformation are finally cleared via an aseptic inflammatory reaction and degradation. This is painful and a common cause of recurrent local symptoms in patients with venous malformations.
Some of these thrombi are not completely cleared, but are palpable through the skin as small nodules of connective tissue. Later they can calcify and form phleboliths.