Chapter: Coagulation disorders
Article: 2 of 6
Update: Feb 24, 2021
Author(s): Wohlgemuth, Walter A.
Depending on the type and size of the vascular anomaly, there are typical kinds of coagulation anomalies associated with vascular anomalies:
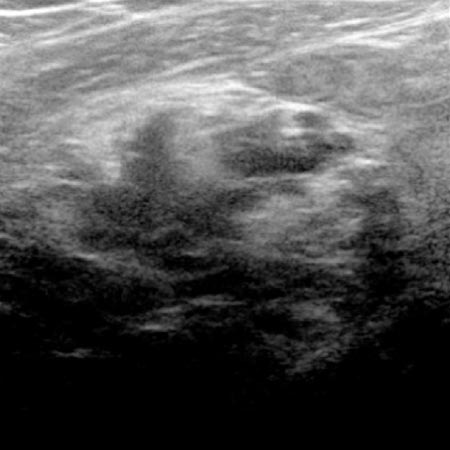
Large venous malformations (VM) in an intramuscular location consist of blood-filled endothelium-lined cavities with dysplastic endothelium and dysfunctional vessel wall in the lesion. The blood contained within shows virtually no flow or complete stasis of the blood. This leads to permanent, ongoing formation of small microthrombi in the form of small blood clots and, at the same time, as a physiologic counterbalance, to secondary activated fibrinolysis. This is expressed clinically as ongoing localized intravascular coagulation (LIC) within the venous malformation. Localized coagulation activation in the vascular anomaly, with thrombin formation and intravascular fibrin deposition, results in counterbalancing secondary hyperfibrinolysis and consumption of coagulation factors, especially the coagulation components fibrinogen, factor XIII, and antiplasmin.
These localized coagulation processes within the venous malformation also give rise to larger local thrombi, leading to frequent painful thrombophlebitis within the venous malformation. Chronic thrombophlebitis results in the formation of phleboliths that are typical of venous malformations. These may arise through normal remodeling processes over time from thrombi that slowly organize during degradation via collagen deposition. These then form a consecutive spherical or popcorn-like calcification (= phlebolith) via an increasing, shell-like attachment of calcium.
The following overview table summarizes the important coagulation phenomena:
| Kasabach-Merritt phenomenon (KMP) | LIC/DIC | |
| Patient | Infant with hard, reddish-bluish vascular tumor | Adolescent/young adult with large-volume VM on extremity or trunk |
| Associated vascular anomaly | Kaposiform hemangioendothelioma (KHE) / tufted angioma (TA) | Venous malformation (VM) |
| Frequency | Up to 45% in the first year of life with KHE/TA | 40%-58% of all patients with very large VM |
| Laboratory constellation | Thrombocytes ↓ ↓ ↓ ↓ D-dimers ↑ ↑ Fibrinogen (↓) | D-dimers ↑ ↑ ↑ Fibrinogen ↓ ↓ Thrombocytes (↓) |
| Cause | Platelet activation at dysplastic tumor endothelium with trapping, secondary clot activation | Activation of plasmatic coagulation by stasis in large, stagnant blood-filled cavities of venous malformation, impaired endothelial function |
| Risk of worsening | Administration of platelet concentrates – immediate consumption, inflammation | Further clot activation due to open surgery, sclerotherapy, trauma, immobilization, etc., – switch to DIC |
| Prophylaxis | Heparin, ASA, possibly ticlopidine | Heparin (already at least 3 days before major planned interventions) |
| Therapy | Transarterial embolization of the tumor, compression therapy, heparin, ASA, ticlopidine, sirolimus, surgery if necessary | Heparin, if necessary Coagulation factor substitution Compression therapy, sclerotherapy and surgery if necessary |