Chapter: Orthopedic problems associated with vascular malformations
Article: 4 of 9
Update: Feb 24, 2021
Author(s): Kertai, Michael Amir
If a joint (often the knee joint) is involved in a vascular malformation, the clinical picture of angiodysplastic arthropathy may develop.
Although this disease has not yet been sufficiently researched in detail, the further course can be predicted by considering other diseases that lead to repeated bleeding or an inflammatory co-reaction in joints (e.g., blood Coagulation disorders). Triggered by an inflammatory co-reaction of the synovium in the case of venous malformations directly close to or in the synovium with recurrent thrombophlebitis, rapidly progressive destruction of the joint on the affected side already occurs at a young age.
Essentially, angiodysplastic arthropathy progresses in phases:
The diagnosis of angiodysplastic arthropathy is based on the patient's Medical history. It is important to ask whether the patient with vascular malformation has ever (or repeatedly) experienced Joint effusion or recurrent inflammation, especially in the knee joint. If the answer is positive, it can be assumed that hemarthrosis or thrombophlebitis close to the knee joint with synovial involvement has occurred.
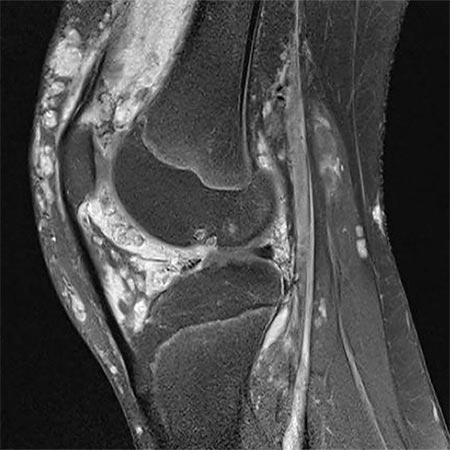
MRI then plays an essential role as a further diagnostic tool, as it can be used to assess a possible Intra-articular extension of the malformation and to detect Hemosiderin residues in the synovium in iron-sensitive sequences in a condition following direct bleeding in the joint.
Specific examinations may still follow in order to plan further therapy.
Actual healing of angiodysplastic arthropathy is only possible as long as destruction of the articular cartilage has not occurred. Therefore, therapy must be started upon first diagnosis of Intra-articular involvement in order to prevent rapid destruction of the joint.
Treatment should always be interdisciplinary. On the one hand, it requires interventional therapy of the peri-articular, or if possible Intra-articular, vascular malformation to close vascular connections into the affected joint and to facilitate surgical access. On the other hand, it requires surgical removal of the peri- and Intra-articular malformation and the altered synovium (Synovectomy), if possible.
Surgical therapy can be either arthroscopic or open. Although the arthroscopic approach has clear advantages in terms of postoperative rehabilitation, it often cannot be used because of the extensive findings and more difficult bleeding control. Essentially, two factors play a role in why an open procedure must often be chosen:
If destruction of the cartilage has already occurred, cartilage replacement therapy must be performed in addition to Resection of the malformation and Synovectomy. However, in most cases this no longer represents a curative approach, but can often only delay the development of osteoarthritis.
As a final therapy, if osteoarthritis is already present, only joint replacement by means of Joint Endoprosthesis is possible.
To summarize, the earliest possible interdisciplinary approach must be advised in angiodysplastic arthropathy, but without compromising on the aggressiveness of the approach because of the young age of most patients. If therapy is too sparing, the patient will have to pay the price later with irreparable joint damage.