Chapter: The classification of vascular anomalies
Article: 3 of 8
Update: June 04, 2021
Author(s): Sadick, Maliha | Wohlgemuth, Walter A.
Simple vascular malformations are mostly composed of a single malformed dominant vascular component: either veins, arteries, capillaries or lymphatic vessels (with the exception of arteriovenous malformations). Based on their flow dynamics, vascular malformations are further subdivided into slow-flow (venous, lymphatic, capillary malformations) and fast-flow (arteriovenous malformations or congenital arteriovenous fistulas) malformations, to which a large number of individual clinical pictures can be assigned. This basic division into slow-flowing malformations (with usually very slow or stagnating flow) and fast-flowing malformations (high shunt volume, warm, pulsating) is very important for the type of therapy to be performed and the long-term prognosis.
Based on the ISSVA classification, the following table provides an overview of the classification of simple vascular malformations.
| Flow dynamics | Vessel component | Clinical picture |
|---|---|---|
| slow-flow | Capillary malformation (CM) |
|
| slow-flow | Lymphatic malformation (LM) |
|
| slow-flow | Venous malformation (VM) |
|
| fast-flow | Arteriovenous malformation (AVM) |
|
| fast-flow | Arteriovenous fistula (AVF) |
|
Abbreviations Table
AVF: arteriovenous fistula, AVM: arteriovenous malformation, CCLA: central conducting lymphatic anomaly, CCM: cerebral cavernous malformation, CM: capillary malformation, CMTC: cutis marmorata teleangiectatica congenita, GLA: generalized lymphatic anomaly, GVM: glomuvenous malformation, HHT: hereditary hemorrhagic teleangiectasia, KLA: kaposiform lymphangiomatosis, , LM: lymphatic malformation, VMCM: familial mucocutaneous venous malformation, PTEN: PTEN hamartoma syndrome
Capillary malformations (CM) account for about 9% of all simple malformations and manifest themselves at birth as circumscribed redness, mainly in the skin or mucous membranes with sharp boundaries to the surrounding tissue. As the growing patient increases in size, they grow proportionally. They consist of dilated, dysplastic capillaries in the skin, which shine through the skin as red spots. The diagnosis can usually be made on the basis of their typical clinical appearance. They manifest themselves as red, sharply delineated maculae of the skin or spots located at the level of the skin. Immediately after birth, they are usually dark red or almost raspberry red in color, may fade somewhat over time or may be associated with mild hyperkeratosis. They persist for life and are occasionally associated with isolated hyperplasia of the affected body region or extremity (diffuse capillary malformation with overgrowth or DCMO) or the underlying soft tissue (especially in the face, cheek and lips with tuberous transformation of these tissues).
Lymphatic malformations (LM) comprise about 15% of all simple vascular malformations. They consist of more or less mature, dysplastic lymphatic vessels and can also form circumscribed, cystic masses. In infants and toddlers, they are conspicuous as circumscribed, usually skin-colored, soft swellings on various parts of the body. They feel soft to the touch since they consist of lymph-filled cystic cavities of varying size.
They manifest themselves as microcystic, macrocystic or combined micro- and macrocystic vascular anomalies. Predilection sites for lymphatic malformations are the head and neck region in 67%, followed by the trunk, chest wall, axilla and extremities in 30%. They rarely manifest themselves in deep tissues or the parenchymatous organs, where they can occur in up to 3%. A special form of lymphatic malformation is the very rare Gorham-Stout syndrome, also known as “vanishing bone disease”, in which lymphatic tissue replaces or destroys bone tissue and can lead to progressive osteolysis. In generalized lymphatic anomaly (GLA), the bones are also affected, but not in such an expansive or aggressive form as in Gorham-Stout syndrome. Internal organs may also be affected in GLA. In central conducting lymphatic anomaly (CCLA), a malformation (hypoplasia, aplasia) of central lymphatic conductors in the abdomen and/or chest causes lymphatic congestion proximal to the stenosis/occlusion. This leads to leg edema, exudative enteropathy, cutaneous lymph vesicles and/or recurrent lymphatic ascites or pleural effusion.
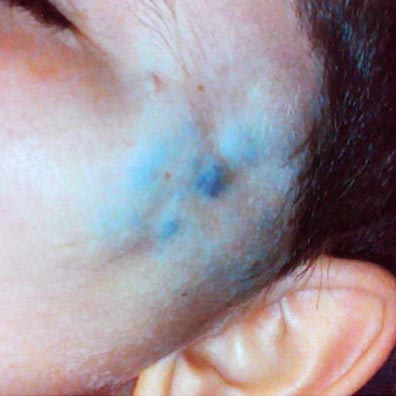
Venous malformations (VM) are the most common slow-flow vascular anomaly, accounting for 70% of cases. They consist of dysplastic, spongy or tubular soft masses, the walls of which are structured like veins and contain blood. They can appear as a small superficial vascular anomaly, often shimmering bluish through the skin, or as an extensive malformation spread to a whole extremity or to organs in almost any part of the body. Venous malformations often cross numerous tissue layers and can extend from the cutaneous to the intraosseous level with correspondingly diverse clinical symptoms. A bluish discoloration of the skin caused by the venous malformation due to malformed cutaneous venous blood-filled spaces can also be an esthetic factor for the affected persons.
Pain and functional limitations are frequent and can be caused by recurrent thrombophlebitis within the dysplastic venous vascular channels.
Arteriovenous malformations (AVM) and the even rarer congenital arteriovenous fistulas make up the smallest proportion of simple vascular anomalies, at approx. 6%. They consist of a malformed vascular area, which in the case of arteriovenous malformation manifests itself most often as multiple, often reticular, direct arteriovenous shunts (nidus), or multiple fine arterial vessels directly connecting to an enlarged draining vein bypassing the normal capillary bed. In the case of arteriovenous fistulas, by contrast, there is a single direct arteriovenous shunt connection. This shunt represents a short circuit of the arterial (inflow) and venous (outflow) vascular system, bypassing the capillary bed. This shunt-related very fast blood flow (fast-flow malformation) often makes the lesions feel warm and even pulsatile through the skin. The skin overlying the lesion is often red. AVMs are among the fast-flow malformations that, depending on their clinical manifestation and biological activity, certainly pose the greatest challenge to patient and physician because they are difficult to treat and often recur.