Chapter: Venous malformations
Article: 2 of 13
Update: Mar 25, 2021
Author(s): Barbera, Letterio Christian
Clinical characteristics of simple venous malformations are:
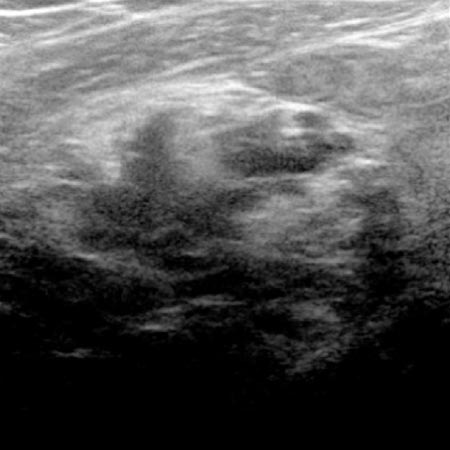
These irregular vascular spaces are filled with blood. Coagulation processes occur within these venous vascular spaces because of stagnant blood with only very slow flow. Therefore thrombi or their calcified residuals (phleboliths) are often visible within a venous malformation.
The sporadic, i.e., non-familial, venous malformation is the most frequent congenital vascular malformation with an incidence of 1–2 in 10,000 and a prevalence of about 1%.
Variable expression: Localization, size, depth and morphology of a venous malformation vary considerably. Each patient shows a very individual pattern, whereby any body area (face, trunk and extremities) and, more rarely, internal organs may be affected. Venous malformations are more commonly localized to the extremities and head and neck region (about 40% each) than the trunk (remaining 20%). A venous malformation is usually limited to one side of the body or one quadrant of the body (e.g. buttocks, leg and foot on one side), although exceptions can occur. The body volume affected by the venous malformation may be limited to a distal phalanx, or can extend to one half of the body. The same is true for the extension in depth: limited to the skin and subcutis only, or possibly involving muscle, bone and joint surfaces. The morphology of a venous malformation can be described as an irregular network of shapeless, spongy or tubular blood-filled vascular conglomerates, which also vary among themselves.
Absence of a regular vessel wall: Venous malformations are not fully matured vessels, thus they do not form a regular wall structure. The wall is usually wafer-thin and valve-less as a result of the malformation. A venous malformation does not look like a vein, but resembles a fox’s den with irregularly distributed blood cisterns of different sizes. Venous malformations are therefore additional, redundant vessels without a transport function, in which the blood accumulates. The consistency of the wall is reminiscent of a spider’s web and ruptures very easily when grasped with tweezers or after puncture.
Increase in volume: Venous malformations change their appearance both during adolescence and in the later stages of life. The reason for this is the immature wall, which increasingly gives way to blood pressure and thus leads to an increase in volume. Thus the total increase in volume is only partly based on cell proliferation and mostly on increased swelling of the blood-filled irregular vascular spaces. The greater the initial volume of a venous malformation, the earlier it appears clinically. On the other hand, smaller venous malformations may only become visible with age. This evolution must be understood and taken into account in the treatment plan.
Combination with capillary and lymphatic vascular malformations: Combined malformations such as CVM and LVM occur more frequently in the extremities. CVMs are more conspicuous and worry parents most because they are easily visible. The red capillary component often fades with growth and usually does not require therapy. However, LVM is clinically more relevant and more difficult to treat.
Association with growth disturbances: Occasionally there is an accompanying partial overgrowth or undergrowth when a limb is affected by a venous malformation. A causal connection in terms of the vascular anomaly influencing tissue growth was previously suspected, but clinical experience and the same genetic mosaics in soft tissue and accompanying vascular malformation did not confirm this. Today, it is assumed that the soft tissue proliferation or diminished growth is directly related etiologically to the malformation of the vessels (combined malformation). These growth disturbances can be accompanied by severe functional limitations. Although the initial difference in length and circumference that occurred in childhood may diminish somewhat with further growth, the treatment plan must take these changes into account.