Chapter: Lymphatic malformations
Article: 6 of 14
Update: Mar 15, 2021
Author(s): Meyer, Lutz
Sonography is the most common and initial method of diagnosis and imaging. It allows classification into microcystic, macrocystic and mixed cystic forms of lymphatic malformation (hereafter “LM”). It provides information on the depth of extension, is used during Sclerotherapy for guidance, and makes it possible to identify and document progression of the disease in the therapeutic process. The Cysts will appear as multiple anechoic, partitioned lesions with a thin wall and multiple thin septa.
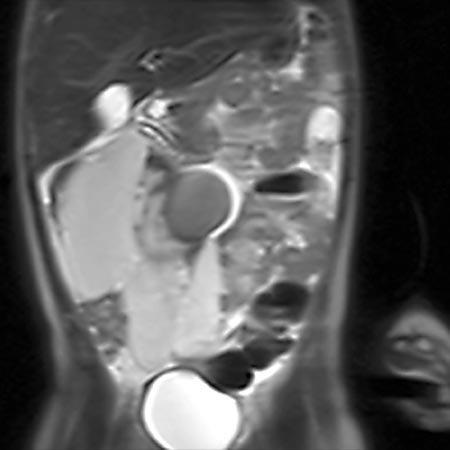
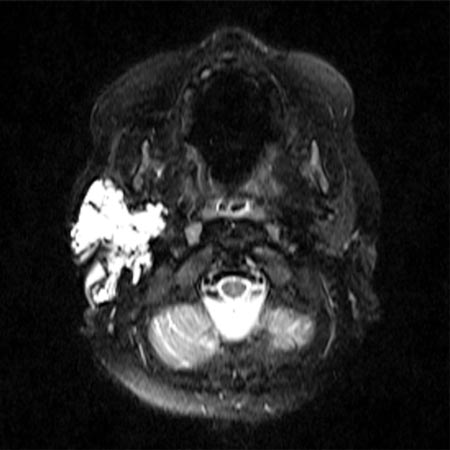
In addition, magnetic resonance imaging is used when there are therapeutic implications or differential diagnostic considerations. It allows better assessment of deeper structures and should be part of the basic diagnostic workup for more extensive lymphatic malformations.
During sclerotherapy, to determine the volume and extension of a punctured LM and to exclude lymphovenous anastomoses, direct radiography (usually as Fluoroscopy) of the punctured lymphocysts can be performed before the sclerosant is injected.
Lymphangiography is again being increasingly used for certain issues. Direct Puncture of lymphatic vessels, e.g., on the dorsum of the foot, or Puncture of inguinal lymph nodes (intranodal lymphangiography), and injection of highly viscous Contrast medium provide radiographic visualization of the lymphatic system and any malformations or lymph leaks.
Computed tomography and survey radiographs are reserved for questions that suggest direct involvement of the bone.