Magnetic resonance imaging (MRI) is a radiation-free imaging method that uses a strong, homogeneous magnetic field (usually 1.5 or 3.0 Tesla) and electromagnetic high-frequency pulses to produce cross-sectional images of the human body. Different tissue contrasts, especially of the soft tissue (fat and water), can be generated by specific changes to the scanning parameters (MRI sequence). According to current knowledge, the examination itself is harmless. Metallic foreign body implants can produce artifacts or heat up, so they must be identified in advance. The selection of the scanning planes and slice thickness depends on the body region to be examined. The examination time is mainly determined by the field of view to be covered and by the number of selected MRI sequences. It typically ranges between 20 minutes and one hour.
Role of magnetic resonance imaging (MRI) in the diagnosis of vascular anomalies
In view of the high soft tissue contrast and the possibility of dynamic vascular imaging (MR angiography), magnetic resonance imaging (MRI) is today the gold standard for evaluation of vascular anomalies and is superior to computed tomography (CT) in many respects, not only because of the lack of use of X-rays. The exact anatomical extension and type of vascular anomaly can be determined with a high degree of accuracy (see table below: Typical MRI findings in vascular anomalies). If a vascular anomaly is suspected and an invasive procedure is discussed, a dedicated MRI should be performed at least once. The basic sequence protocol includes non-enhanced T1-weighted fast spin-echo sequences without fat suppression and T2-weighted sequences with fat suppression (STIR). The latter is extremely fluid-sensitive and is therefore very well suited as a “search sequence” for the detection of venous and lymphaticvascular malformations. In addition, T2-weighted fast spin-echo sequences without fat suppression are helpful. Special T2* and T2-FLAIR sequences have a role in the imaging of vascular malformations in the central nervous system. After application of gadolinium MRI contrast agents, T1-weighted sequences with fat suppression (e.g., 3D) are acquired. The administration of contrast agents can also be used to perform time-resolved MR angiography (MRA).
Typical findings
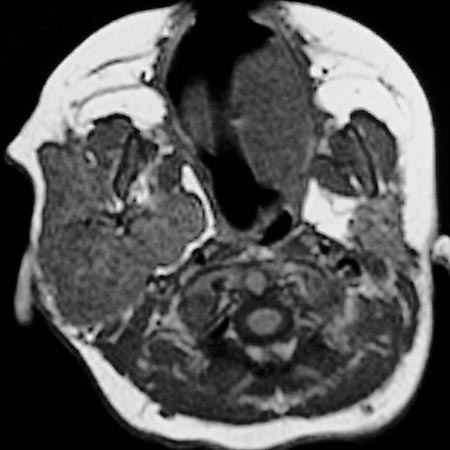
Infantile hemangioma: In the proliferation phase, infantile hemangiomas appear hypointense to isointense in non-enhanced T1-weighted sequences and strongly hyperintense with sharp margins in T2-weighted sequences. Flow voids in the incoming and outgoing vessels indicate a high blood flow. After administration of contrast medium, proliferating infantile hemangiomas enhance early, intensely and homogeneously and are sharply demarcated. However, there is no immediate arteriovenous shunting as in true arteriovenous malformations. During the involutional phase, the increased fat deposition leads to a signal increase in T1-weighted sequences. The contrast medium uptake is reduced.
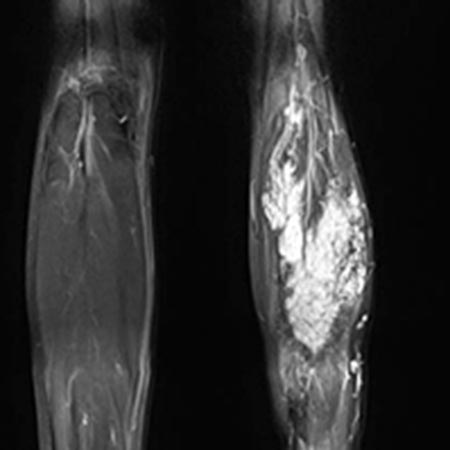
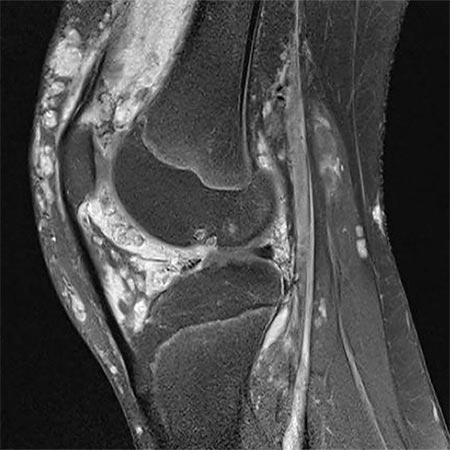
Venous malformation: In T2-weighted sequences, a strongly hyperintense signal predominates, which is highly visible on fat-suppressed T2-weighted sequences (STIR). Here they appear as septated, lobulated sponge-like or tubular masses, but often without any real space-occupying effect. Usually, venous malformations are isointense to the surrounding musculature on non-enhanced T1-weighted sequences. Spherical structures within the lesion with low signal on all sequences correspond to thrombi or calcified phleboliths which are pathognomonic for venous malformations when intralesional. Fluid-fluid levels can also be observed due to sedimentation phenomena within the venous malformations, but these are less frequent than in lymphatic malformations. After application of contrast medium, venous malformations slowly enhance contrast medium homogeneously. The average time to full contrast agent enhancement is about 90 seconds, which is significantly longer than for arteriovenous malformations (< 5 seconds). In contrast to arteriovenous malformations, in venous malformations the arteries supplying the affected extremity are not dilated. Flow voids are missing in venous malformations. Therapy-relevant venous connections (communicating veins) between the venous malformation and the deep venous system are occasionally identifiable on MRI. Abnormalities such as aplasia or hypoplasia of the deep and superficial venous system are also detectable.
Lymphatic malformation: The cysts of a macrocysticlymphatic malformation are predominantly iso- to hypointense on native T1-weighted sequences. A different protein content and deposits after bleeding lead to fluid-fluid levels within the cysts or to a homogeneously increased signal intensity. Sometimes accompanying dilatations of veins can be detected in lymphatic malformations. Similar to venous malformations, lymphatic malformations show a strongly hyperintense signal in fat-suppressed T2-weighted sequences (STIR). The septa and walls of macrocysticlymphatic malformations can enhance contrast medium while the cyst content typically shows no contrast medium uptake.
Arteriovenous malformation: The morphologic correlate of the arteriovenous malformation, the so-called nidus (network of direct arteriovenous shunts), is often very hard to detect on native MRI sequences as a solid component is missing in AVMs. Occasionally, the AVM is surrounded by edema or connective and fatty tissue. Typically, spin-echo sequences (T1 or T2) show flow voids within the vessel channels because of high flow velocity. Diagnosis can ultimately be made with the help of dynamic MR angiography with high spatial and temporal resolution. Here, the nidus and the dilated, draining veins are contrasted almost immediately via the corkscrew-like dilated arterial feeders. In lesions located in the extremities, the inflowing and outflowing vessels are usually significantly enlarged compared to the unaffected side. In some cases the vessels are degenerated and show aneurysmal dilatations (so-called flow-related aneurysms). On account of the shunt with low flow resistance, normal vessel sections distal to the shunt may no longer be visible on MRA because of a steal phenomenon. The tissue surrounding the nidus typically does not show contrast enhancement and is hardly recognizable as the actual lesion since the lesion lacks a solid component. However, after invasive procedures or during an inflammatory or proliferative phase, surrounding edema with contrast enhancement is occasionally visible.
Typical MRI findings in vascular anomalies
Description
T1-SE
T2-STIR
MRA (TWIST)
T1 fat-sat after Gd (late phase)
Vascular tumors
Infantile hemangioma
Well-defined, solid space occupying lesion
Hypointense to isointense
Flow voids
Hyperintense
Flow voids
No real AV shunts
Homogeneous enhancement (proliferative phase)
Vascular malformation
Slow-flow
Venous malformation
Septated lobulated masses with little space-occupying effect
Thrombi, phleboliths
Isointense (muscle)
Fluid-fluid level
Hyperintense
Fluid-fluid level
Very slow CM pooling
Patchy enhancement
Lymphatic malformation (macrocystic form)
Cystic space-occupying lesion
Iso- to hypointense
Fluid-fluid level
Hyperintense
Fluid-fluid level
Not visualized
Cyst content without enhancement
Occasionally enhancement of the cyst wall/septa
Fast-flow
Arteriovenous malformation
Nidus barely visible on non-enhanced sequences
Dilated vessels (inflow and outflow)
Flow related-aneurysms
No solid component
Nidus barely visible
Dilated vessels
Flow related-aneurysms
Flow voids
Nidus barely visible
Dilated vessels
Flow related-aneurysms
Flow voids
Immediate contrast enhancement of the nidus
Immediate contrast enhancement the draining veins
Flow related-aneurysms
Dilated inflow and outflow vessels
Flow related-aneurysms
Disadvantages
The numerous different MRI sequences sometimes add up to long examination times (up to 45-60 minutes) depending on the body region. For some patients the MRI examination may be accompanied by feelings of anxiety or claustrophobia, and there is a high noise level (earplugs may be necessary). Patients with claustrophobia may sometimes require appropriate sedation. In infants and small children, a time-consuming MRI can only be performed under general anesthesia. A prerequisite for the application of an MRI-specific contrast medium is a satisfactory kidney function and exclusion of other contraindications. Furthermore, before each MRI examination, it must be ensured that no ferromagnetic foreign materials are in contact with the body or have been implanted in the body.
13-year-old girl with severe cartilage damage in the knee joint due to extensive peri- and intra-articular venous malformation; therapy with surgical synovectomy and cartilage replacement
2-year-old girl with large, space-occupying mass on the right neck that increased immediately after birth and did not regress (infantile hemangioma); embolization therapy