The following remarks refer to experience with children and adolescents in pediatric hand and foot surgery. The initial therapy of all vascular malformations is conservative. All therapeutic indications should be coordinated on an interdisciplinary basis.
Principles of surgical therapy
Indications for surgery in vascular malformations are pain, bleeding, recurrent infections and functional impairment caused by the size and bulk of the malformation. In older children, improving the contours and thus the appearance by tissue reduction on the finger and back of the hand is another reason.
The management of vascular malformations is sometimes discouraging and frustrating for surgeons because they are usually not completely removed surgically and can recur. The postoperative outcome often cannot be estimated beforehand with certainty. For extensive tumor-like lesions, the goal of surgery is limited to contributing to mass reduction and thus alleviating symptoms. In view of the special anatomy of the hand with its important functional structures in close proximity, such as nerves, vessels and tendons, it is difficult or impossible to remove the malformations without permanent damage in the case of extensive findings.
Observing the following principles helps to achieve the best possible results in surgical therapy:
Preoperative planning: The three-dimensional extent and location of the malformation must be compared with the clinical findings and the diagnostic imaging. If all tissue layers have been penetrated by the malformation, flap plasty for reconstruction must be planned preoperatively. According to the motto “Keep it simple”, a local flap procedure should be preferred to free flaps from distant sites, if possible.
Informed consent: All possible complications must be discussed with the parents, including blood loss, bruising, possible skin defects, infections, neuroma, tendon adhesions, joint stiffness. In the case of very extensive severe arteriovenous malformations, amputation should be discussed, especially if the distal part of the limb is affected.
Surgery under optical magnification: Surgery under magnifying glasses is mandatory in order to see and preserve all important nerves, tendons and muscles. A surgical microscope is needed to restore vessels during revascularization.
Surgery in a bloodless state: Only in a bloodless state can surgical preparation be carried out quickly and precisely, thereby sparing nerves and vessels. In addition, blood loss is minimized. Before the wound is closed, the tourniquet should be opened and bleeding carefully stopped.
Incisions: The end phalanx of the finger should be incised laterally and longitudinally, the finger by a palmar zigzag approach according to Bruner and dorsally through a curved longitudinal incision, running longitudinally along the forearm.
If a multi-step procedure is required, the malformation is resected as completely as possible within a circumscribed area in each step. Combined dorsal and palmar or radial and ulnar surgery on both sides of the finger simultaneously should be avoided owing to the risk of circulatory impairment.
The aim is complete removal to avoid reoperation in the scarred area in the case of recurrence, as reoperation in a scarred region is risky.
Ultrasound dissection allows for a more radical and gentle operation, especially in the case of venous malformations.
If nerves are also affected, intraneural dissection should be avoided because of the risk of neuroma formation.
In distal ischemia of fingers, revascularization with venous interposition is always part of the planned reconstruction.
It is pointless to preserve marginally perfused finger areas by flap surgery.
Joint stiffness is common in large venous malformations as a result of intra-articular expansion and bone involvement.
Venous malformations
Venous malformations (VM) and mixed malformations (LVM) are the easiest to treat surgically. Venous malformations (VM) usually extend wider than the clinical impression suggests.
Surgical indication:
Circumscribed extent
Pain
Deterioration of function
Desire for cosmetic improvement
Circumscribed venous malformations
Circumscribed venous malformations are very amenable to surgical treatment. The goal is complete removal while preserving functional structures. Resection can achieve a high level of general patient satisfaction, satisfaction with the appearance and pain reduction.
Damage in the form of premature closure of the epiphyses and joint malposition can be caused by VM or its treatment.
Venous malformations at a functionally important site
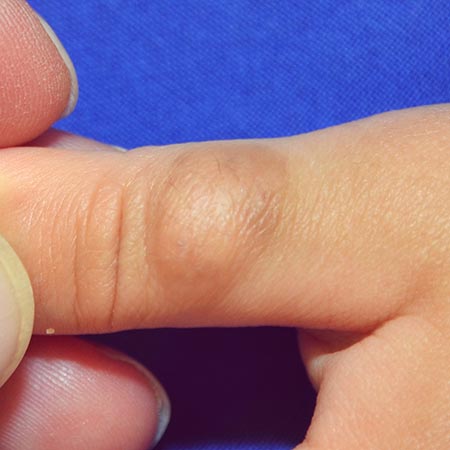
Circumscribed venous malformations at functionally important sites are difficult to treat. The VM in this two-year-old patient only extends to one part of the thumb, but the sensitive thumb pad is affected, which is important for grasping. In this case, ultrasound dissection has proven to be helpful. However, a recurrence within 15 months could not be prevented. A second ultrasound dissection is planned via a fish mouth incision with distalization of the excess skin and resection of the distal pad-like parts. A conceivable alternative would be resection of the entire thumb pad or interventional therapy. For reconstruction, the entire palmar distal phalanx would have to be replaced by a sensitive microvascular partial big toe transplant. Even after this complex therapy, recurrence is possible.
Extensive venous malformations on the finger, hand and forearm
If complete resection is not possible, sclerotherapy is a good treatment option. Surgical therapy is only indicated for problems that cannot be controlled with compression and sclerotherapy. Combinations with preoperative sclerotherapy to reduce the size of the findings are also possible. Local excisions are helpful for painful venous ectasia and nerve compression. Large venous ectasias are less well tolerated on the finger than on the rest of the arm. Deep venous malformations on the forearm, in the elbow or on the upper arm are usually located next to the neurovascular structures and extend along the fascia. They often extend into the musculature. An impairment of growth is usually observed in combined malformations with a venous component. Ulcerations are rare. Sclerotherapy is often recommended for large VMs for treatment or to prepare for a planned resection 4 to 6 weeks preoperatively. Close cooperation between the disciplines involved is necessary for establishing the indication and planning. In the case of intra-articular extension, damage to the joint surfaces is to be feared. In this case, surgical therapy is the only remaining option.
In the case of very extensive diffuse venous malformations, surgical therapy is not indicated if the patients are pain-free. This is the domain of conservative therapy or interventional therapy.
Resection with an ultrasound dissector is helpful because it allows for a much more radical and gentle operation with fewer adhesions. Ultrasound dissection has proven its worth in liver surgery over the past decades. High-frequency ultrasound waves are generated in a transducer and cells are fragmented by cavitation. Soft tissues such as tumors, parenchyma and fat are easy to fragment. Structures with less fluid such as vessel walls, nerves, tendons and ligaments are resistant to fragmentation. They are protected by the ultrasonic waves. The recurrence rate also seems to be lower: In a personal communication Guero reports a recurrence in 15 cases after 1.5 years following surgery without ultrasound dissection and in 33 patients after 5 years with ultrasound dissection.
Lymphatic malformations with venous parts
Lymphatic malformations (LM) occur as circumscribed space-occupying cystic masses and/or as circumscribed, often extensive lymphedema. The most common combination in the case of vascular malformations is a combination of lymphatic and venous dysplasia (LVM). Preoperative MRI diagnosis is often helpful for smaller circumscribed lesions of the finger or hand with lymphatic parts. They should be removed as completely as possible if surgery is intended. If the skin is infiltrated, it must be resected as well. If the peritendineum is preserved, the defect can be covered by skin graft. If vessels or tendons are exposed after resection, local flap surgery is indicated (cross-finger flap or heterodigitally vascularized island flap from an adjacent finger). During resection, no more than half the circumference of a finger or hand should be operated upon in one session.
Lymphatic malformations that extend over the entire arm usually displace nerves and muscles. Infections with ß-hemolytic streptococci without a visible entry point frequently occur. The therapy of these erysipelas is conservative. Surgery, as in the case of extensive venous malformations, is only indicated if location, size, weight and macerations are very severe. Patients are less often affected by pain, but more by infections and local lymphorrhea with soaking of clothing and the resulting odor nuisance.
Drainage attempts by microsurgical anastomosis between lymphatic vessels and veins have not so far been successful. Amputation may be considered in cases of massive expansion and non-functional extremities.
Arteriovenous malformations
Arteriovenous malformations (AVM) are characterized by continuous arteriovenous shunting in the nidus, increase in nidus size, venous dilatation and pulsations. Surgery or trauma can induce an uncontrolled increase in size. Therefore, caution should be exercised before surgical interventions. Deterioration is possible as a result of the surgery.
Arteriovenous malformations differ in the hand from venous malformations in terms of clinical signs, complaints, extent and number of fistulas. The clinical picture plays a decisive role in the decision for or against surgical therapy.
Patients with only mild symptoms, with AVM of circumscribed size, good function and low pain level should be treated conservatively.
Patients with moderately severe symptoms, with moderate AVM size and marked functional impairment and severe pain can be treated conservatively or by embolization.
Patients with pronounced symptoms, massive extension, severe ischemia, steal phenomenon with gangrene, recurrent massive bleeding, nerve compression or compartment syndrome and/or cardiac decompensation have a high surgical risk. However, severe pain and cardiac impairment are considered absolute indications for interventional or combined open operative therapy.
Foot
Mixed vascular malformations often occur as capillarylymphatic-venous malformations (CLVM) in the context of circumscribed tissue hyperplasia. Well-known examples are Klippel-Trénaunay syndrome with capillary and venous (+/- lymphatic) malformations and skeletal overgrowth, and CLOVES syndrome (Congenital Lipomatous Overgrowth, Vascular malformations, Epidermal nevi, Skeletal anomalies). The majority of these overgrowth forms affect the lower extremity. The aim of treatment is to make life easier for those affected by ensuring painless feet and enabling them to wear a ready-made standard shoe of the same size as the other foot.
Establishing the indication and performing the surgical resection requires a lot of experience in this situation, especially when looking at the long-term course.
The feet can be surgically narrowed by means of ray resection. Prominent parts are resected if they cause pressure sores. We know from malformation surgery that walking in preschool children is not impaired by resection of one of the middle rays. After resection of the complete ray, the deep metatarsal ligament is reconstructed with 3-0 or 4-0 PDS sutures.
Length overgrowth of the foot can be limited by open or percutaneousepiphysiodesis. The timing of this operation depends on the length of the foot of the same-sex parent. In upright X-rays with a measuring scale, the length of the individual limbs on both sides is measured and compared to the parent. After the age of 10 to 12 years, epiphysiodesis is no longer useful as there is only little residual growth to align for discrepancies.
18-month-old child with slow-growing, slightly bluish mass on the thumb. Primary resection with skin grafting due to unclear provenance of the enlarging mass; histology: venous malformation