Chapter: Invasive therapy
Article: 10 of 15
Update: Feb 07, 2021
Author(s): Barbera, Letterio Christian
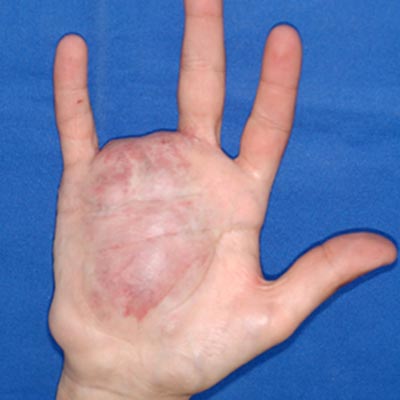
Open surgery on the limbs is most commonly performed in venous and less frequently in arteriovenous and lymphatic malformations. The former are more common and are surgically easier to approach. In arteriovenous malformation (AVM), the greatly increased vascularization of the tissue results in a bloody and therefore unclear surgical field, which increases the rate of complications (bleeding, nerve injury, ischemia) and reduces the effectiveness of incomplete resection.
Arteriovenous malformations consist of innumerable, tiny arteriovenous fistulae that are not visible to the naked eye, so that preparation and targeted ligation are not possible. Surgical resection may still be useful if the arteriovenous malformation is localized on a finger or toe or if complete embolization is performed and resection will reduce residual swelling or symptoms.
In this case, the possibility of a combined therapy with prior embolization and subsequent resection of the occluded nidus should also be mentioned. Based on knowledge of vascular and hand surgery, it is possible to remove the malformation-bearing tissue in a bloodless state. The procedure is time-consuming, so that only one phalanx of a finger or toe should be approached per surgical session.
If the arteriovenous malformation is located more proximally, repeated embolization of the vascular nidi is the better procedure.
Although lymphatic malformations (LM) also occur in the extremities, they rarely cause mechanical complications requiring resection. The removal of skin areas with microcystic lymphatic malformations to prevent recurrent inflammation is associated with wound healing disorders and many recurrences and has therefore rarely proven to be effective.
Venous malformations (VM) are more suitable for open surgery than arteriovenous malformations and lymphatic malformations. Although smaller venous malformations can be adequately treated by one treatment, a large number of patients require repeated procedures.
Surgical treatment is particularly important for symptomatic, voluminous vascular malformations, which often occur in the subcutis on the lateral side of the lower and upper leg. The surgery of venous malformations is fundamentally different from varicose vein surgery and places special demands on the surgeon. The venous stripping that is common in truncal secondary varicosis would cause severe bleeding and only insufficiently correct the malformation. The vulnerable vascular wall, irregular borders, varying caliber, extension across tissue layers, adhesions with the surrounding tissues due to recurrent thrombophlebitis and the abundance of blood in the adjacent soft tissues are special features of open surgery in congenital vascular malformations and require large accesses as well as meticulous and time-consuming preparation.
Special caution is required in the presence of a lymphatic malformation, especially lymphedema. After identification and preoperative marking of the clinically relevant parts on the body, visualization and circular dissection of the vessel convolutes are performed through long enough skin incisions.
Side branches and deep connections are directly ligated or treated with suture ligatures. The large-caliber malformations can thus be removed with little blood loss. The required careful preparation of an area of 5 x 5 cm can take up to an hour, which must be taken into account when planning the procedure.
Similar to sclerotherapy, it is therefore advisable to address a few highly painful sections instead of resecting the malformation throughout the entire length of the leg, for instance. A circumscribed and stepwise resection is particularly necessary in cases of simultaneous aplasia or dysplasia of the deep venous system, as the venous outflow of the limb might otherwise be endangered. The surgical manipulation of larger areas of venous malformation can also trigger disseminated intravascular coagulation (DIC) with subsequent bleeding that is difficult to stop. For this reason, it is advisable to measure blood levels of D-dimers in extensive venous malformations and, if necessary, to combine preoperative anticoagulation with intra- and postoperative coagulation substitution.
The benefit of resection of subfascially located venous malformations must be questioned in view of the increased risk of bleeding, insufficient resectability, muscle and nerve damage, and an inadequate benefit-risk ratio for transfascial extension. The immature vessels in the muscular compartment are very thin-walled and tend to rupture. An isolated, complete dissection is rarely possible, so that one is often forced to resect the entire muscle tissue containing the malformation.
However, surgery may represent a safe and effective therapeutic procedure if these precautions are observed (preoperative measurement of D-dimers + fibrinogen and, if necessary, anticoagulation, resection of only circumscribed areas, avoidance of subfascial VM). The procedure concludes with particularly meticulous hemostasis and layered and tension-free wound closure. Compression bandages, elevation of the extremity and cooling have a pain-relieving and decongestant effect. Depending on the size and location of the wounds, mobilization is performed early (if necessary on crutches) and is accompanied by analgesia as needed.
The duration of the inpatient stay depends on the degree of postoperative mobilization, which may vary depending on the findings and the patient. In most cases, the clinic can be left after 2-4 postoperative days, although follow-up care must be well organized. The patient, family and resident colleague providing aftercare need detailed information about the postoperative care, level of exercise allowed, and wound care. In typical malformation patients, the young age and the absence of relevant comorbidities mean that complications in the postoperative course are fortunately rare.
If the indication and handling are correct, surgical resection complements the other invasive treatment procedures in such a way that they can be used in combination in some cases. This applies to preoperative sclerotherapy for venous and lymphatic malformations and preoperative embolization for arteriovenous malformations.