Chapter: Thrombosis and thrombophlebitis
Article: 2 of 4
Update: Mar 24, 2021
Author(s): Wohlgemuth, Walter A.
Thrombophlebitis consists of a circumscribed, localized inflammation of a superficial vein or venous cavity within a venous malformation (VM) caused by a fresh intravascular thrombus. The local inflammatory reaction usually occurs aseptically without involvement of infectious agents, as a result of the organizing remodeling of a blood clot with corresponding release of inflammatory mediators.
These changes, typical of patients with venous malformations, are circumscribed, relatively sudden in onset, only a few centimeters in size, locally painful, palpably indurated, and may recur at various sites. They are usually not dangerous. Particularly in patients with larger venous malformations, they occur more frequently in phases, sometimes even at sites that previously did not externally appear to be affected. They usually regress on their own within a few days. Practically all patients with venous malformations are affected by localized painful thrombophlebitis in the course of their lives.
Little is scientifically known about the mechanisms of the development of thrombophlebitis. The initial cause is circumscribed blood clot formation within a superficial vein or within a venous malformation.
All factors that increase the blood's ability to clot, such as dehydration, hormones, immobility, nicotine abuse, oral contraception, infections, surgery, interventions, wounds, congenital thrombophilia, etc., favor the formation of such blood clots. Slow blood flow in the veins (this is especially true for venous malformations which are slow-flow lesions) and damage to the venous vessel wall (also common in venous malformations with dysplastic vein walls) also favor the development of blood clots in a vein. This can then develop into painful thrombophlebitis, but the dissolution of the local blood clots can also go clinically unnoticed.
The onset of fibrinolysis, which is always activated in the presence of an intravascular thrombus, releases inflammatory mediators, including leukotrienes, interleukins, and complement factors. When this inflammatory response is disproportionately severe, clinically painful thrombophlebitis results.
Thrombophlebitis occurs in a circumscribed way either in a strand-like pattern along a vein or as sudden, painful, usually raised indurations a few centimeters in size. Corresponding to an inflammation, this may be accompanied by local redness and hyperthermia. Thrombophlebitis is almost always painful to touch and pressure.
Thrombophlebitis usually occurs only in clearly circumscribed areas and measures a few centimeters in size. If somewhat deeper, the swelling or discoloration may not be visible, and there is only a circumscribed finding that is initially painful to palpation. In the course of life, virtually all patients with venous malformations are affected. Thrombophlebitis is the most common cause of their pain.
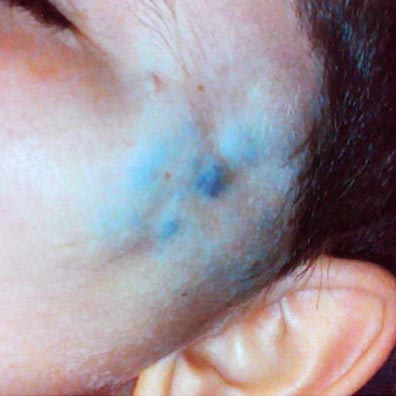
When superficial, thrombophlebitis may also look like a circumscribed hematoma appearing translucent through the skin. In this situation regression of thrombophlebitis is accompanied by changes in its color like a typical hematoma: initially dark bluish, then reddish and yellowish, then gone after a week.
The diagnosis is usually made clinically. The sudden circumscribed appearance, symptoms, and underlying venous malformation make the diagnosis clear.
Laboratory chemistry focuses on the elevated D-dimers, which are fibrin degradation products produced during fibrinolysis of the clot. However, in many patients with venous malformations, especially those with larger-volume malformations, elevated D-dimer levels are detectable throughout life. Thus, thrombophlebitis cannot be detected by this measure alone.
If imaging is ever necessary, sonography is the first choice. Thrombophlebitis is easily visualized within the anechoic venous malformation components as echogenic, non-compressible circumscribed foci.
On sonography, a normal vein or venous malformation is soft and readily compressible with the transducer. The non-clotted blood is virtually anechoic (black), and slow blood flow is detectable on color-coded duplex sonography.
As the blood clot matures with time, it becomes more echogenic sonographically, making it easy to distinguish from anechoic blood. Often starting at the edge, i.e., at the vessel wall, there is a slow recanalization of the involved vessel. This is visible as anechoic fluid around the echogenic thrombus.
In ultrasound elastography, thrombi tend to be harder than the surrounding tissue. Therefore they are also relatively easy to detect according to the color scaling setting.
Thrombophlebitis is also depicted in direct phlebography or varicography (in the context of therapy). Intravascular thrombi present themselves as local non-contrasted areas within a vessel. Thrombophlebitis per se is not an indication for phlebography.
Because of their frequency, especially in venous malformations, acute thrombophlebitides are often visualized incidentally in magnetic resonance imaging (MRI) as part of treatment planning, since this imaging is often performed in symptomatic patients. Thrombophlebitis per se is not an indication for MRI. The fresh thrombi present as hypointense (black) in T2-weighted images as compared to the very hyperintense (white) venous malformation. In T1-weighted imaging, they vary in signal intensity and may be isointense or slightly hyperintense to the blood in the surrounding venous malformation. As a result of the inflammatory reaction of the thrombophlebitis, there may be significant local enhancement after contrast administration; in fat-saturated T2-weighted imaging, surrounding edema can then also be visualized.
Thrombophlebitis is painful for some time (typically a few days) but is usually harmless in itself. Only if the swelling becomes severe can local compression symptoms occur.
It is important to know whether patients with larger venous malformations have venous communications draining to the deep conducting venous system. If these connections are present and have a large lumen, clinically relevant blood clots may drain off from the venous malformation and cause thromboembolism with thrombosis and / or pulmonary embolism. Detection of these connections (from VM to deep venous system) is best accomplished with direct phlebography. If detected, these communicating veins should be occluded.
A rare complication of thrombophlebitis is additional bacterial superinfection, which occurs mainly in patients with concomitant lymphatic malformations in the sense of combined venolymphatic malformation. Clinically this situation presents as a rapid local escalation of inflammation and pain, which may also be accompanied by fever and systemic signs of inflammation. Antibiotics may be indicated in such cases; always consult a physician.
The most important therapy is local treatment of the inflammatory reaction. Local cooling, elevation to relieve pressure, and, if necessary, analgesic and anti-inflammatory ointments (e.g., diclofenac gel) are the standard therapy. Local compression that is not too strong can accelerate regression, especially in the subacute phase.
Only exceptionally, in cases of severe pain or pain persisting for several days, therapy with low-molecular-weight heparin in a prophylactic dosage for 5 to 7 days helps to achieve rapid improvement. Alternatively, direct oral anticoagulants can be taken for a few days.
If thrombophlebitis recurs locally at a similar or the same site, which may also limit activities of everyday life, invasive therapy may be warranted, whether sclerotherapy or open resection of the affected parts of the venous malformation.
The most important prophylactic measure is appropriate compression therapy. Compression reduces the volume of the cavities of the venous malformation. Thus fewer thrombi can form within the congested, blood-filled dysplastic venous vascular spaces, and hence thrombophlebitis is less likely to occur.
All circumstances that increase blood coagulability should be avoided (see above). Regular exercise is necessary, especially during prolonged periods of immobility (e.g., driving, travelling, computer work). Prolonged standing and sitting without intermittent exercise should be avoided.
Prophylactic anticoagulation because of recurrent thrombophlebitis is only necessary in very rare cases. In such cases, invasive therapy such as sclerotherapy of the affected lesions is more likely to be useful in the long term. However, low-dose or, in rare cases, even therapeutic anticoagulation for days to weeks may be useful as an acute therapy.
An important indicator of recurrent thrombophlebitis in the past may be the number of phleboliths present within the venous malformation (e.g., seen in ultrasound or X-ray). As a rule of thumb, the more frequently thrombophlebitis occurred in the past, the more frequently phleboliths are detectable. Patients with multiple phleboliths are more often symptomatic and also benefit from invasive therapy.