Chapter: Histology
Article: 5 of 6
Update: Feb 04, 2021
Author(s): Evert, Katja
A purely histopathologic differentiation of the different vascular anomalies is difficult without clinical data. Nevertheless, many lesions show a relatively characteristic appearance. The morphologic description in combination with the corresponding immunohistochemical markers, aided by clinical and imaging data, enables a differential diagnosis to be made in most cases for the lesions presented below.
Arteriovenous malformations are biologically locally relatively aggressive malformations which have a tendency to recur and even proliferate when only small remnants are present. They consist of numerous malformed arteries, veins and capillaries with direct connection between arteries and veins (arteriovenous shunts). However, it must be said that these arteriovenous shunts are very difficult to detect directly by histology. Clinically, they present in a variety of ways depending on their location: they can appear as red, warm, pulsatile masses, they can lead to ulcerations and venous hypertension. A very large shunt volume can lead to cardiac overload.
Histologically, large veins and arteries and small blood vessels in a fibrous or fibromyxoid stroma are visible. The arteries and veins are structurally malformed and sometimes have very thick walls with clear fragmentation of the elastic fibers. The formation of arteriovenous shunts is very difficult to detect in histologic specimens. As a result of the increase in pressure, the veins show very thick walls with widening of the intima, while veins in other sections can also become very thin-walled and dysplastic in some cases.
Capillary malformations are most commonly found on the skin and mucous membranes. They are present at birth and can be recognized as pink to red spots. They usually persist for life, some variants can become lighter or recede completely, usually by the age of 10.
Capillary malformations consist of dilated capillaries and/or post-capillary very small veins in the upper dermis, which become visible through the skin. Over time, there is sometimes increasing vascular dilatation which makes them appear darker and histologically produces a nodular, plaque-like image. They may be associated with other vascular and non-vascular anomalies, in which case they are combined malformations.
Venous malformations (VM) usually present as blue discoloration of the skin or as a soft subcutaneous mass when in a superficial location and can generally affect any tissue or organ. As a rule, they are soft to the touch, compressible lesions that tend to increase in size and volume. This can lead to changes in the venous pressure system.
Venous malformations are lesions with ill-defined margins in which veins of different sizes and different structures are found. In some cases they show very thick walls with fibrosis of the adventitia, but in other cases very thin malformed vascular walls as well. The malformed veins can lie close together, but they can also be very loosely distributed in the stroma. Glomuvenous malformations represent a special form in this context. These are typically small, bluish, usually painful lumps. They show a typical histology of blood vessels whose vessel wall is surrounded by multiple layers of glomus cells.
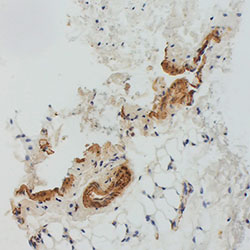
Lymphatic malformations (LM) are made up of numerous dilated, dysplastic lymph vessels, some of which are so massively dilated that they form lymphatic cysts. A distinction is made here between different forms of these cystic changes:
Very clear rules for the exact differentiation do not exist; in general, macrocystic LM cysts are considered to be larger than 1 cm. One point that may help differentiate is the practical question of whether cysts can be punctured and therefore sclerotherapy can reduce the size of the lesion. In H&E staining multiple dysplastic endothelial spaces are seen, normally without erythrocytes and very thin walls. In immunostaining these endothelial cells express D2-40 (podoplanin), which gives them a brown lining under the light microscope as a sign of their lymphatic origin.
Infantile hemangiomas are proliferating vascular tumors with an antigenic structure similar to that of placental tissue. Local or regional tissue hypoxia is discussed as a potential pathogenic factor in their development. They must be distinguished from other vascular tumors, e.g., kaposiform hemangioendothelioma (KHE) or pyogenic granuloma, and from arterial, venous, lymphatic or combined malformations of the vascular system. Histologically, this is possible by immunohistochemical detection of GLUT1, among other things. In the clinical context, histologic examination is often not necessary because the diagnosis can readily be made from the clinical presentation and the radiological findings.
Infantile hemangiomas typically appear in the first days or weeks after birth.
There are precursor lesions such as circumscribed teleangiectasias, pale, reddish or bluish maculae or nevus flammeus-like changes. However, an infantile hemangioma never manifests itself as a tumor at birth.
There are three different stages in the development of infantile hemangiomas:
The histologic presentation varies depending on the developmental stage of the lesion, but a clear, definite differentiation of the different phases is not possible histologically. In the early growth phase, the image is dominated by plump endothelial cells and pericytes with a bright cytoplasm, which form narrow capillaries with barely visible lumens. Cellularity is very high, so that it can be difficult to detect the actual vascular differentiation. Mitoses are also found at this stage.
As the disease progresses, the picture changes. The lumens become wider and the endothelial cells flatter. This process often starts at the border of the lesion and then spreads towards the center.
In the involution phase, the blood vessels recede as the lesion becomes increasingly fatty.
These are rare vascular tumors which, in contrast to infantile hemangiomas, are already fully developed at birth and do not proliferate.
Histologically lobular capillaries separated by connective tissue can be seen; these are often accompanied by atrophy of the skin appendages. The capillaries partly contain plump endothelial cells and pericytes, which may look very similar to the proliferative phase of an infantile hemangioma, but here the proliferation rate (Ki-67) is very low. In addition, the vascular endothelia of congenital hemangiomas are negative for GLUT1. For further clinical description of congenital hemangiomas please refer to the chapter “Vascular tumors”.
Kaposiform hemangioendothelioma (KHE) is a locally aggressive tumor often associated with a Kasabach-Merritt phenomenon and it occurs almost exclusively in childhood (more than half of the cases occur in the first year of life); in adulthood these tumors are very rare. They occur most frequently in the soft tissue of the extremities, and a small percentage may also occur in body cavities. As a rule, the tumors are ill defined, violet-blue-red in color.
The tumors consist of irregular vascular nodules that diffusely infiltrate the soft tissue (“cannon-ball” fashion) and are occasionally accompanied by stromal desmoplasia. Areas that resemble a hemangioma and also Kaposi’s sarcoma can be found within the tumor. An essential characteristic is the formation of glomeruloid structures consisting of very dense, CD31-positive capillaries with actin-positive pericytes. Fibrin thrombi are frequently found here. Another special feature is the frequent presence of lymphatic vessels, corresponding to lymphatic malformation parts, within a KHE. This becomes visible through vascular endothelia positive for D2-40.
Angiosarcomas are malignant mesenchymal tumors that originate from the endothelium. They can develop at any age but, unlike most vascular anomalies, the highest incidence is in the seventh decade of life. In childhood, however, they are very rare. The etiology is unclear in most cases, while some are associated with radiation exposure or chronic lymphatic congestion. They often develop in the deep muscles of the extremities (approx.
40%), but they can also develop in the retroperitoneum, mediastinum or mesentery.
Clinically, angiosarcomas are painful, reddish nodular masses, often associated with other symptoms such as coagulopathy, anemia or persistent hematomas.
Histologically, angiosarcomas are very diverse. In addition to areas with almost regularly formed blood vessels with only slight atypia of the endothelia, solid cell clusters or spindle cell areas with strong atypia are also prominent. Mitoses may be increased, and sometimes necroses are also seen. Excessive bleeding may mimic the image of a hematoma, so that a careful histopathologic work-up is necessary.
Kaposi’s sarcoma is a locally aggressive endothelial tumor or tumor-like lesion that usually manifests itself as multiple skin lesions, but can also affect mucous membranes, lymph nodes or other organs.
Kaposi’s sarcoma is uniformly associated with infection with human herpesvirus 8 (HHV 8). This can be visualized with the specific immunostaining.